
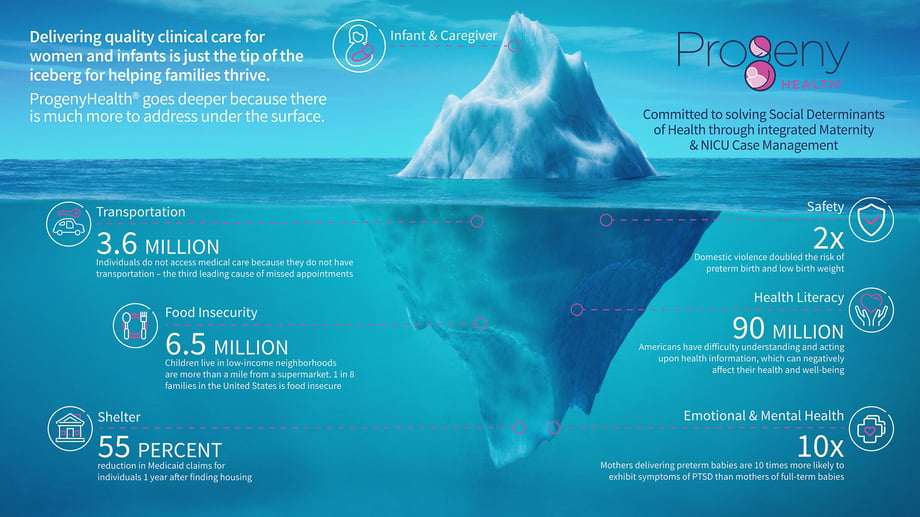
The word “health” describes our physical condition, but it is also a reflection of how we live. Where we were born, how we learn, work, shop, play, and age all affect our quality of life. These health-influencers are called Social Determinants of Health (SDoH).
SDoH issues affect what we eat, our sense of security, social engagement, and family support. They can enhance or degrade our well-being by affecting access to healthcare, fresh food, and a living space free from toxins and other physical threats. Solving for the broad array of SDoH needs is critical to maintaining a continuity of care for women, infants, and their families – across both Medicaid and commercial health plan populations.
The integration of Utilization Management (UM) and Case Management (CM) enables collaboration, coordination, and communication across multiple clinical disciplines and departments – and with local social resources and services. Incorporating SDoH into the clinical ecosystem facilitates healthy outcomes for women and infants by helping families address the problems that impact their daily lives.
The Social Determinants that affect families include:
Health Literacy
A new parent or caregiver’s health literacy – the capacity to obtain, interpret, and understand basic health information – can affect their ability to follow recommendations to safeguard infants from illness or injury and promote their well-being. Studies indicate that 90 million Americans have difficulty understanding and acting upon health information, and, that this issue is compounded when language barriers are involved.
Twenty percent of caregivers in one study demonstrated low health literacy and had difficulty managing services. Supporting and educating caregivers to achieve a higher level of health literacy helps them communicate with providers more efficiently and navigate the support system and resources they need.
Food Insecurity
1 in 8 Americans faces food insecurity. 6.5 million children live in low-income neighborhoods that are more than a mile from a supermarket. Children who live in households that are food insecure are likely to be sick more often, recover from illness more slowly, and be hospitalized more frequently. Food insecurity can affect children in any community, not only traditionally underserved ones.
 Emotional Health/Mental Health
Emotional Health/Mental Health
1 in 8 of all visits to US emergency departments are related to mental and substance use disorders. Parents are at particular risk for postpartum depressive symptoms, anxiety, and stress after their newborns are discharged from the hospital
Shelter
Infants born during a period of unstable housing have higher rates of low birth weight, respiratory problems, fever, and other common conditions. They also experience longer neonatal intensive care unit stays, more emergency department visits, and higher annual spending.
As cited in this article, one study found a 55 percent reduction in Medicaid claims for individuals one year after finding housing, and others have also shown that access to stable housing shortens hospital stays by 29 percent and reduces emergency department visits by 24 percent.
 Community
Community
Where you live matters to your health. 80% of health outcomes are impacted by socio-economic conditions, health behaviors, and one’s physical environment. Additionally, studies show that integrating social/community services with medical services can be ten times more effective than waiting for families to visit health services.
Transportation
The availability and accessibility of public transportation impact access to employment, healthy food, health care, and other drivers of health and wellness. The American Hospital Association reported that 3.6 million individuals – regardless of payer status – are unable to access medical care because they lack transportation.
Interpersonal Safety
Domestic violence by a partner or ex-partner during pregnancy increases the risk of preterm birth, low birth weight, and small-for-gestational-age babies. This risk is increased further for women who experienced two or more types of domestic violence during their pregnancy.
Data indicates a direct correlation between SDoH and infant mortality (IM). Studies reported in the Journal of Health Care for the Poor and Underserved show:
- Poverty – Individuals with the lowest incomes have the highest risk of infant death. For example, African Americans and non-Hispanic Whites in the highest poverty tier are at greater risk of sudden infant death syndrome (SIDS). Poverty has also been shown to be a contributor to acute and chronic stress, which have an impact on infant mortality.
- Breastfeeding – Studies found that breastfeeding for any duration decreased the likelihood of SIDS.
- Education – Several studies have found education to be a protective factor against infant mortality. The odds of infant mortality were higher for non-Hispanic Black women with low levels of education than for their non-Hispanic White counterparts.
- Maternal Health – Multiple studies have demonstrated the increased risk of infant mortality from maternal conditions such as diabetes and hypertension.
- Smoking – Maternal smoking in the prenatal and postpartum periods increases infant mortality. Second-hand smoke in the infant’s environment is also associated with an increased risk of infant death, including unexplained infant death (SUID), SIDS, and infectious diseases.

- Safe Sleep – Unsafe sleep positions (i.e., prone position) increase the odds of infant mortality and are particularly associated with increased risk of SIDS. Some segments of the population are less likely than others to follow physician recommendations. Access to cribs and bassinets is another SDoH factor in sleep-related infant deaths.
- Access to Healthcare – Rural areas and poor neighborhoods often have few medical specialists, such as obstetricians and neonatologists. Residing in a region with more specialists lowers the risk of neonatal mortality. The level of hospital care also plays a significant role, especially the quality of healthcare facilities. One study found that African American women who deliver in NYC hospitals have overall higher infant mortality rates.
- Social & Environmental Factors – Neighborhood poverty and racial segregation are associated with higher rates of infant mortality. Family imprisonment rates increase infant mortality, as does income inequality. Exposure to air pollution (i.e., carbon monoxide, nitrogen dioxide, and fine particulate matter) in the months preceding an infant’s death was significantly associated with infant mortality.
 ProgenyHealth’s Utilization Management, Case Management, and Payment Validation and Assurance programs are tightly integrated into a comprehensive solution to serve infants, families, providers, payers, and employers.
ProgenyHealth’s Utilization Management, Case Management, and Payment Validation and Assurance programs are tightly integrated into a comprehensive solution to serve infants, families, providers, payers, and employers.
Our proven Process, technology Platform, and our experienced team of People enable our partners to reduce NICU case costs and sustain those savings post-discharge by identifying and solving SDoH issues impacting these families.
Our Process:
From pregnancy to a potential NICU admission, through the first birthday and beyond, our focus is on infant health outcomes and the well-being of families/caregivers by engaging in collaborative care conversations with providers and affirming standardization of care that follows recognized best practices.
-
-
Utilization Management: Our UM team monitors the infant’s progress telephonically and maintains contact with the hospital staff, forging strong peer-to-peer clinical relationships with them to evaluate and help ensure the quality and efficiency of the care being delivered.
-
Case Management: Our case managers advocate for the infant by engaging with the caregiver and providers to develop an integrated and holistic plan of care. The clinical case managers support the family by assessing, coordinating, and educating, while also considering the family’s unique physical, social, and cultural needs. A key element addressed by the case manager is solving for social determinants of health issues specific to each family’s situation. Our CM team helps NICU families prepare for their transition to home -- typically connecting with the family within 48 hours of admission into the NICU. We conduct a needs assessment before the infant’s discharge and continue to assess the ongoing clinical needs of the infant throughout the first year of life, including the identification of SDoH issues facing the family. The assessment serves to inform the member-centric plan of care which supports the interventions used by our case managers to solve for any clinical and SDoH issues present throughout the first year.
-
Throughout the entire maternity journey, we support members via voice calls, emails, and text to help ensure a safe, nurturing environment. Our CM team serves as a 24/7 lifeline for support, facilitating access to primary care, answering questions, providing education and appointment reminders, and making connections to community resources to solve SDoH issues.
Our Platform:
We manage the entire continuum of care through Baby Trax®, our purpose-built platform for medically complex infant care that integrates UM, CM, SDoH, and clinical best practices. Using proprietary protocols developed over 16 years and 71,000+ cases, Baby Trax provides a single source of truth for ProgenyHealth’s NICU Care Management program. Baby Trax supports clinical workflows by integrating EHR case data with evidence-based guidelines, prescriptive analytics, and flagging inconsistencies through real-time predictive analytics.
![]() Shelter
Shelter
Solve housing challenges, help apply for housing assistance and for infant Social Security Disability Income
![]() Health Literacy
Health Literacy
Obtain vital resources like breast pump, car seat, and crib; lactation support, behavioral health resources, wellness rewards
![]() Food Insecurity
Food Insecurity
WIC benefits and food stamps, local food banks and faith-based programs
![]()
Transportation
Schedule transportation for initial and ongoing doctor’s visits
![]()
Emotional & Mental Health
Ongoing postpartum care visits, continued screening for signs of depression, connect to social workers
![]() Safety
Safety
Obtain authorization from state custody offices, monitor prescribed Medication-Assisted Treatment (MAT)
![]() Community
Community
Integrated medical and social services are more effective than waiting for families to visit health services
 Progeny Health’s data-driven Baby Trax platform, coupled with intensive case management and social worker interventions, enables at-risk infants and their caregivers to overcome the most complex SDoH issues. Here’s an example:
Progeny Health’s data-driven Baby Trax platform, coupled with intensive case management and social worker interventions, enables at-risk infants and their caregivers to overcome the most complex SDoH issues. Here’s an example:
Stella and Beatrice – Born at a fragile 26 weeks, premature twins, Stella and Beatrice, needed significant time in the NICU to grow, sleep, and become medically stable. The twins were born during the COVID-19 pandemic to Patricia, a certified nurse’s aide with two toddlers at home. Adding to Patricia’s challenges, the dad was unable to return to the U.S. from overseas due to travel restrictions. Needing to care for her toddlers and avoid her job-related risks from COVID-19, Patricia had no income to create a stable home for her newborns.
Case Management – Our CM team secured rent assistance which freed up rent money for the purchase of food and supplies. Our team also engaged community resources for infant care items, cribs, car seats, and more.
Results – With these pressures lessened, the family was able to better care for their toddlers and devote necessary attention to the care of the preemie twins. This family's story is unique, but they are certainly not alone.